An introduction to Leucine Metabolism: Isovaleric Acidaemia (IVA)
This introduction guide to Isovaleric Acidaemia (IVA) helps parents and carers to understand and manage the condition.
This is an introduction to Isovaleric Acidaemia (IVA) which is an example of a disorder of leucine metabolism, which will be the focus of this resource.
Following the diagnosis of your child with this condition. Consult your metabolic team for diagnosis and treatment for IVA.
This is not designed to replace any advice given by the metabolic team at the hospital.
If you are unclear about anything written on this page, please ask your dietitian for further information.
This page was written with Prof Anita MacDonald who is a metabolic dietitian from Birmingham Children’s Hospital, who has over 40 years of experience working with parents/carers and children with IVA.
What is IVA?
Isovaleric Acidaemia or IVA for short
It is pronounced iso-val-eric-acid-ur-eea.
If left untreated, chemicals in the blood build up to toxic levels.
This can cause a range of symptoms such as poor feeding, vomiting, dehydration, lethargy, floppy infants, excessively sleepy, rapid breathing, unpleasant smell in urine, seizures, coma and brain damage.
IVA can be life threatening if left untreated.
In newborn infants diagnosed with IVA, if treated early and effectively children with IVA can do well and improve long-term outcome.
Diagnosis of IVA
This blood test (heel prick test) is carried out by a healthcare professional after birth.
High levels of a chemical called isovaleric acid are found in the blood.
Diagnosis is confirmed with further blood and urine tests.
Once diagnosed the child will be referred to a specialist metabolic centre to ensure they receive the care they need.
Why does my child have IVA?
IVA is an inherited genetic condition
It’s nobody’s fault and there is nothing you could have done to prevent it.
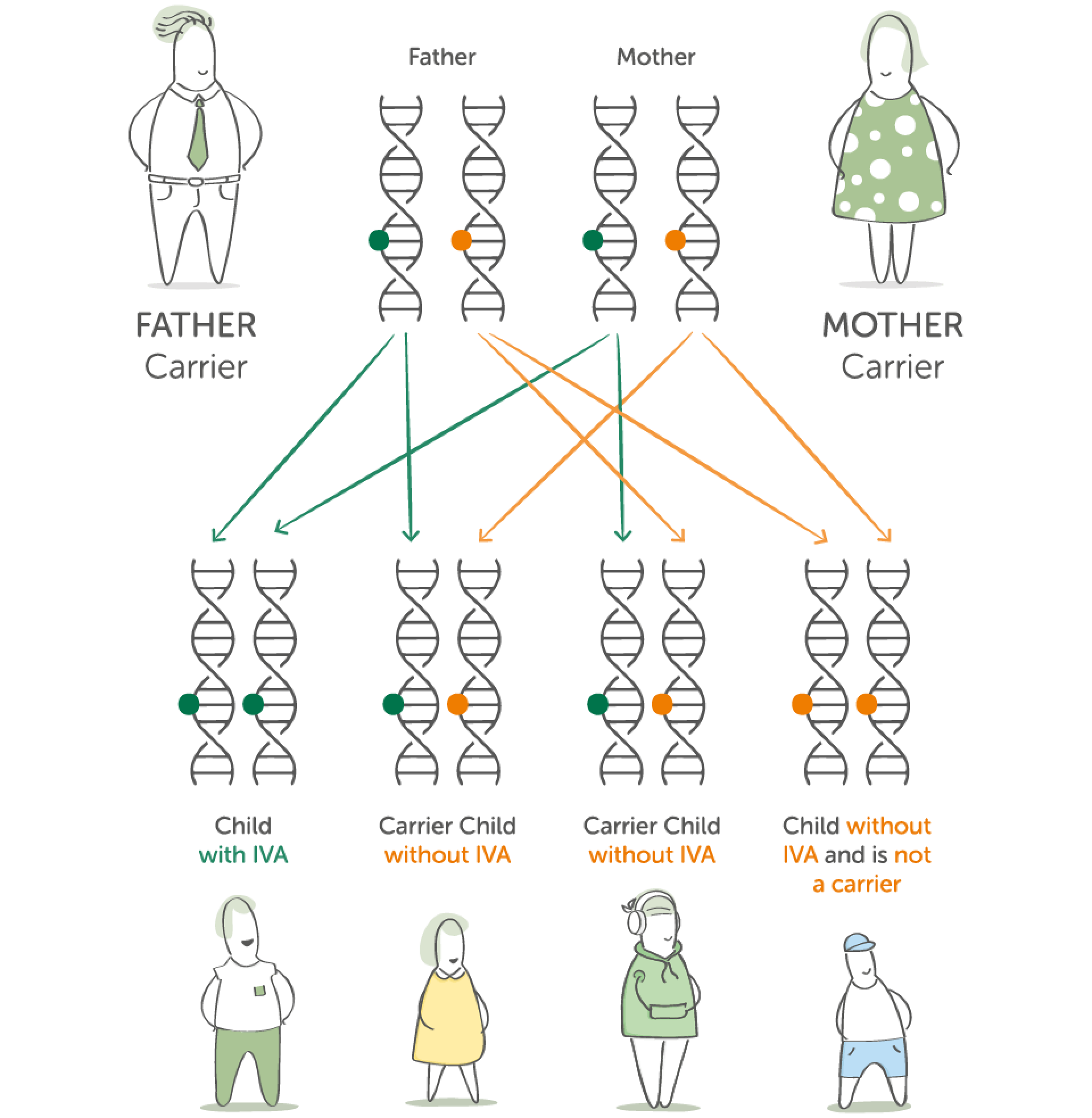
As a parent of a child with IVA, you have one IVA gene and one unaffected gene.
This is known as being a carrier.
For a child to inherit IVA, it requires both parents to be carriers of the IVA gene.
Your child has inherited 2 IVA genes, one from the father and one from the mother and so therefore has IVA.
There are a small number of people who are carriers of the IVA gene
People who are carriers for IVA do not have IVA themselves and in fact do not normally know they are carriers. The IVA gene does not cause a problem to them.
When 2 people who are carriers of the IVA gene conceive a child there is a 1 in 4 chance of that child having IVA.
The science bit... Protein explained
Why do we need protein?
Protein is one of the nutrients needed by the body.
It helps to build, repair and maintain body cells and tissues, like your skin, muscles, organs, blood and even bones.
Protein is made up of different building blocks called amino acids.
When it is eaten it is broken down into these amino acids so they can be absorbed into the blood stream and travel to where they are needed.
The conversion of protein into amino acids
Enzymes are special proteins which are like chemical scissors needed for the breakdown of protein into amino acids. There are 20 amino acids (building blocks) that make up protein.
Protein
Enzymes
Amino acids (Building Blocks)
Leucine is one of these amino acids and is used by the body to make new chemicals.
It is leucine that a person with IVA cannot process correctly.
Why can someone with IVA not process leucine correctly?
A person without IVA
Leucine
IVD Enzyme
Isovaleric Acid
Energy + growth + repair
Normally the liver produces an enzyme called isovaleryl-CoA dehydrogenase (IVD) which helps breakdown leucine into isovaleric acid other useful chemicals for the body.
A person with IVA
Leucine
Faulty/No IVD Enzyme

Buildup of isovaleric acid and other harmful chemicals
In IVA the IVD enzyme is either not made by the liver or it does not work properly.
This causes isovaleric acid and other harmful chemicals to build up and become toxic to the brain.
Management of IVA…
- A protein restricted diet
- Medications – such as glycine and carnitine
- An Emergency Regimen during illness
Diet Management
A typical diet has too much protein and therefore leucine for a person with IVA.
It is important that enough protein is given for growth and development, but not too much as harmful chemicals will be made.
Therefore they must follow a moderate protein restricted diet.
The diet will typically be made up as follows:
- Half - foods very low in protein
The remaining:
- Third - dairy based protein (i.e. yoghurt, cheese and milk)
- Third - cereal based protein (i.e. cereals and rice)
- Third - plant based protein (i.e. peas, sweetcorn and potatoes)
Measured amounts of protein
Your dietitian will advise you how much protein your child will tolerate.
This will depend on the severity of the condition.
These foods need to be measured and taken everyday.
They will mainly come from dairy, cereal and plant based foods.
Your dietitian will teach you how to measure protein.
They will provide you with a list of foods suitable for your child.
Low protein foods
Most fruit and vegetables such as, peppers, grapes, carrots and tomatoes can be eaten freely.
These foods should make up the majority of your child’s diet.
They provide an important source of energy and variety in the diet.
Your dietitian will provide you with a list of foods suitable for your child.
What is a protein substitute?
Why does a person with IVA need to take a protein substitute?
Due to the protein restricted diet, some individuals may be unable to get all the nutrients they need by food alone. They may need to take a protein substitute*.
A protein substitute is a specially made medical supplement.
It is leucine free, but it contains all the other amino acids in protein that your child needs to grow and develop.
Most protein substitutes also contain vitamins, minerals and other important nutrients to ensure your child is getting what they need.
If your child requires a protein substitute, your dietitian will discuss this with you in more detail.
* Protein substitutes designed for the dietary management of GA1 are Foods for Special Medical Purposes which must be used under medical supervision.
Management during illness
Emergency Regimen (ER)
As with all infants and children, illness will occur from time to time.
However, those with IVA will need to start a special feed called the emergency regimen (ER) as soon as illness starts. DO NOT DELAY.
The ER is made up of a glucose polymer and a protein substitute.
Your child’s metabolic team will provide an emergency regimen specific for your child and will teach you in advance about what to do in times of illness.
This is an extremely important aspect of dietary management.
When your child gets ill, contact your child’s metabolic team immediately and keep in regular contact with them.
If symptoms continue and/or you are worried, go to the hospital immediately.
An ER can help minimise the impact of illness on your child.
Any common childhood illness or infection can cause glutaric acid levels to rise - avoidance of this is essential.
If left untreated, it can become life threatening.
The ER supplies energy and protein substitute to prevent a buildup of these harmful chemicals.
Always make sure you have your ER products and a written emergency plan - check that the products are in date.
During illness – start the ER promptly – do not delay
- Stop all protein in food and drink temporarily.
- Always complete the full amount of the emergency feed.
- Continue on medication as directed by your doctor.
- Maintaining your infant’s fluid intake during illness is important and extra fluid may be necessary.
- Keep in regular contact with your metabolic team.
How will I feed my newborn?
Infants: breastfeeding
Your infant may be given a leucine free formula alongside breastfeeds.
You will be advised by the dietitian on how much of each of the formula and breast feeds to give.
Your dietitian will advise you on this in more detail.
Breastfeeding offers many benefits for infant and mother; it is recommended you discuss this with your healthcare professional.
Infants: non-breastfeeding (Bottle feeding)
Your infant may be given a leucine free formula alongside the standard infant formula.
You will be advised by the dietitian on how much of each of the formulas to give.
Your dietitian will advise you on this in more detail.
Introducing complementary feeding
When to start introducing complementary feeding
Complementary feeding is often referred to as weaning. It is the process of gradually introducing solid foods into your infant’s diet. Your dietitian will advise you when to start solid foods, but it will occur around the same time as infants without IVA.
First foods introduced will initially be low protein foods.
This will help your infant to develop a healthy eating pattern while eating a variety of foods.
Your infant needs to continue to take their leucine free formula and breast milk/standard infant formula as advised by their dietitian.
7 to 12 months
Once your infant is accepting low protein foods, some foods containing measured amounts of protein are introduced.
Over time, your child will get more of their protein from food (e.g. cereal) and replace the protein they were getting from breast milk or standard infant formula.
Your child will also be encouraged to move to more textured food and finger foods to encourage self-feeding.
Your infant will also begin to drink from a beaker.
Your dietitian will provide more detail about introducing complementary feeding.
Monitoring
You and your child will need to attend your specialist metabolic centre to meet with the metabolic team for ongoing monitoring and check-ups.
At your child’s monitoring visits, the team will spend time with you to ensure your child’s condition is being well managed and tailored to best suit the needs of your child and family.
To do this they look at many different factors such as:
- Your child’s overall health, growth and well-being.
- Blood tests - blood results give a good indication on how well your child is doing.
- Your child’s nutritional intake - it is helpful to bring diet diaries to your clinic visits.
Your dietitian and doctor will discuss any changes that may be needed to your child’s diet or medication.
It is very important to attend these monitoring visits. They will also give you opportunities to discuss concerns or questions you might have.
As your child grows up
Children / Teenagers / Adults
Following the prescribed diet, medication and acting quickly at times of illness ensures the best chance of improving long term outcome.
Download to share offline
Want to digest this information offline? A illustrated version of this pages is ready for you to download and keep.


