What is Cow’s Milk Allergy (CMA)?
Cow’s Milk Allergy (CMA), also referred to as Cow’s Milk Protein Allergy (CMPA) is the abnormal response by the body’s immune system towards the Proteins found in cow’s milk, dairy products and other ruminant milks. On first expose to these dairy proteins, which can occur via the skin, or via the oral or nasal cavity, the immune system is ‘sensitised’ meaning antibodies (called IgEs) associated with dairy proteins are present in the body (1). On subsequent oral exposure to dairy the babies’ immune system recognizes these proteins as harmful and through these IgE antibodies initiates the release of natural defence substances, such as histamine, which lead to the allergic symptoms that are seen. These reactions are usually rapid, within minutes to ~2 hours (2), and can in rare cases be severe, leading to anaphylactic shock. Anaphylactic shock is the most severe form of food allergy but only affects a very small number of children (<0.001%) (3). There is another type of CMA which involves other immune cells, called non-IgE-mediated CMA. Non-IgE-mediated CMA tends to be less severe but takes longer to present itself (from 48 hours to weeks) and is therefore harder to diagnose. Finally, there are also mixed forms of CMA, combining both IgE antibodies and other immune cells.
Prevalance
CMA is one of the most common food allergies presenting in early childhood (4, 5). It affects ~2-3% of infants (4) but varies between regions and countries. Luckily however, most children outgrow their allergy by about 3 to 5 years of age (80-90%) (6, 7, 8).
How is it diagnosed?
The diagnosis of CMA is made by performing a thorough food allergic history, IgE testing when IgE mediated CMA is suspected, and in some cases an oral food challenge (OFC) is needed. IgE testing can include Skin Prick Tests (SPT) or specific IgE antibody tests (sIgE).
When non-IgE-mediated CMA is suspected then food exclusion followed by food reintroduction is the only reliable method to diagnose.
How is it managed?
The management of CMA should always be under medical supervision. The mainstay of management is to remove the implicating protein, in this case Cow’s milk proteins or dairy proteins, from the diet. In breast fed babies who are allergic to dairy, the advice is that the mother should remove dairy from her diet but should continue to breast feeding. In such cases the mother may need supplemental calcium and vitamin D, which should be discussed with the dietitian or treating doctor. Breast fed babies are less prone to CMA that formula fed (ref), and breast milk provides all the nutrients a baby needs, regardless of their condition. In formula fed babies or babies that are taking formula and breast feeds, there are a range of specialist products available to replace standard infant formula. These are called hypoallergenic formula (low allergenic feeds), and they have been tested and proven to be safe to use in infants with CMA. These hypoallergenic feeds can be either extensively hydrolysed formulae (eHFs) of animal or plant origin, or can be amino acid-based formulae (AAFs). Partially hydrolysed formula are not recommended for the management of CMA.
What kind of products are used for the Management of CMA?
There are two different types of hypoallergenic infant formula, used for the management of CMA:
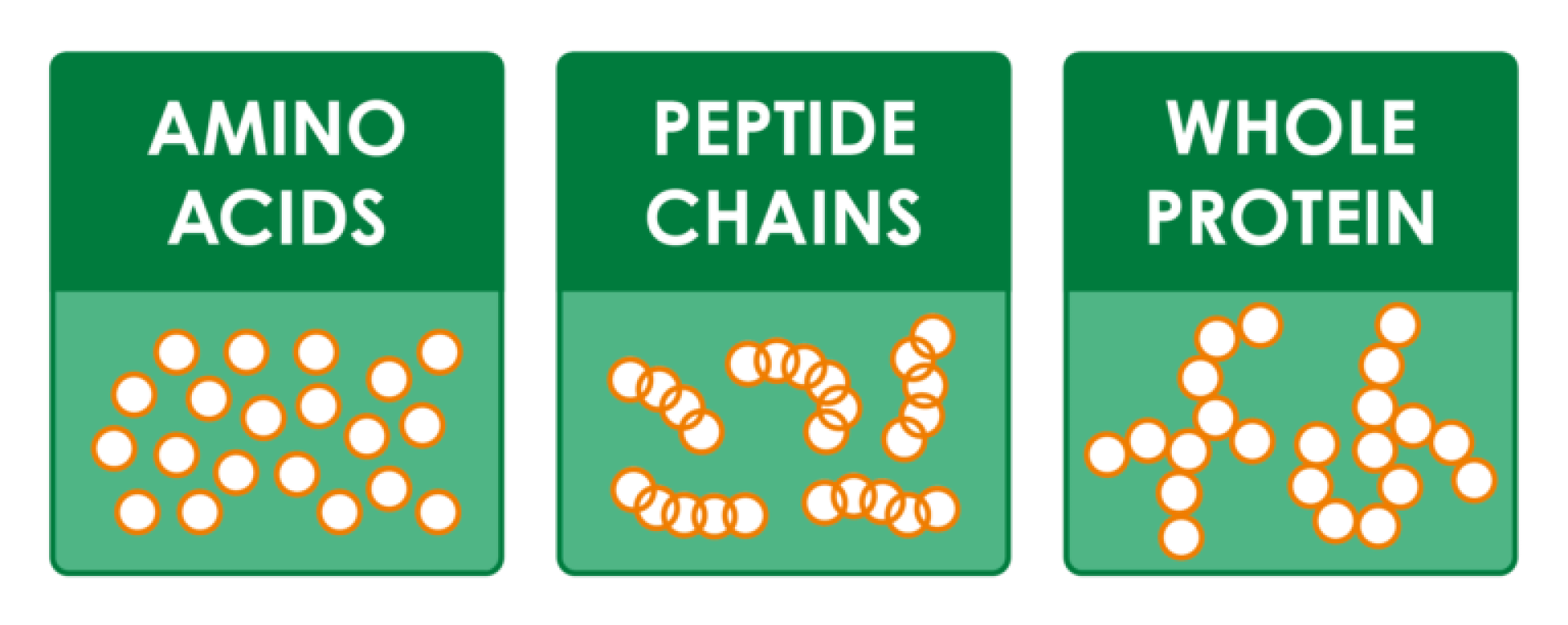
eHF – extensively hydrolysed formula means the proteins are broken down so that the immune system does not recognize them as allergic. They are also called pre-digested feeds. These formulae are the first line treatment for most CMA cases. However, when there has been an anaphylactic reaction to cow’s milk proteins or dairy products, then an AAF should be used.
AAF – amino acid formula is where the protein is fully broken down to individual amino acids so there are no protein chains. These are 100% free of any cow’s milk protein and are therefore the one feeds that are considered are recommended for children anaphylactic reactions to cow’s milk products or failure on an eHF. In some centres they also suggest AAF as first line treatment for some non-IgE-mediated CMA, such as eosinophilic oesophagitis (EOE).
All products should be used under medical supervision.
When do children outgrow their CMA?
Most children outgrow their allergy by about 3 to 5 years of age (80-90%) (6, 7, 8). When exactly a child outgrows their allergy is very much dependent on the original severity of the CMA, and the type of CMA. There are two main types of CMA, IgE-mediated and non-IgE-mediated but there can also be a mix of these two. IgE-mediated CMA tends to take longer to outgrow than non-IgE-mediated CMA. Your doctor or dietitian should advise if further allergy testing or an OFC is needed. These are usually performed in hospital clinics, although in when the risk is considered very low they are carried out in the home.
References
- (1) Venter, C., Brown, T., Meyer, R. Walsh, J., et al. Better recognition, diagnosis and management of non-IgE-mediated cow’s milk allergy in infancy: iMAP—An international interpretation of the MAP (Milk Allergy in Primary Care) guideline. Clin. Transl. Allergy 2017, 7, 26.
- (2) Vandenplas Y, Al-Hussaini B, Al-Mannaei K, Al-Sunaid A, et al. Prevention of Allergic Sensitization and Treatment of Cow’s Milk Protein Allergy in Early Life: The Middle-East Step-Down Consensus. Nutrients. 2019 Jun 26;11(7).
- (3) Cianferoni A, Muraro A. Food-induced anaphylaxis. Immunol Allergy Clin North Am. 2012 Feb;32(1):165-95.
- (4) Sicherer SH. Epidemiology of food allergy. J Allergy Clin Immunol 2011; 127:594-602.
- (5) Canani RB, Nocerino R, Terrin G, Frediani T et al.: Formula Selection for Management of Children with Cow’s Milk. Allergy Influences the Rate of Acquisition of Tolerance: A Prospective Multicenter Study. J Pediatr 2013;163:771-7.
- (6) Levy Y, Segal N, Garty B, Danon YL. Lessons from the clinical course of IgE-mediated cow milk allergy in Israel. Pediatr Allergy Immunol 2007; 18:589-93.
- (7) Høst, A., Halken, S., Jacobsen, HP., Christensen, A.E. et al. Clinical course of cow’s milk protein allergy/intolerance and atopic diseases in childhood. Pediatr. Allergy Immun. 2002, 13, 23–28.
- (8) ASCIA 2019: https://www.allergy.org.au/patients/food-allergy/cows-milk-dairy-allergy

